Proteomics and Its Clinical Application
How proteomics offers opportunities for understanding complex diseases, like cancer.
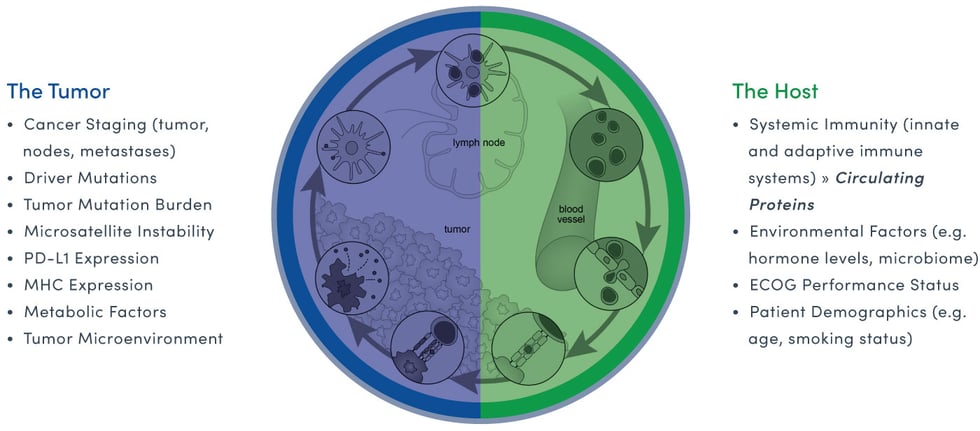
Interpreting the cancer ecosystem offers a clear example of how genomic and proteomic data combine to provide clinically valuable intelligence. While genomic data uncovers the potential genomic drivers of cancer (tumors in particular), proteomic data profiles the patient’s (or host’s) immune response to the cancer. Both are critical elements for interpreting the real-time complexity of the cancer disease state or cancer ecosystem.
The easiest way to understand why it’s important to study the genome and the proteome for the best clinical outcome is through the simple analogy of a caterpillar morphing into a butterfly. Both have identical genomes but vastly different proteomes. This enables the caterpillar to crawl from place to place and the butterfly, the ability to fly.
Similarly, cancer-cell to host-cell interactions create a new, complex environment, that when properly understood, can directly inform clinical decisions based on the real-time status of the cancer ecosystem.
Since its emergence and subsequent acceleration following the completion of the Human Genome Project, proteomics has given rise to a new set of methodologies, techniques, and technologies to aid in understanding, detecting, and treating diseases like cancer by characterizing the protein networks that both control and are controlled by the information encoded by the genome. (Srinivas et al, 2002)
All of these tools and methods, as Srinivas et al explain, must contend with challenges unique to the study of proteins. These include the inherent complexity of protein regulation, difficulties in capturing protein targets given the specific determinants of their behavior, and the task of detecting low-abundance proteins given that the dynamic ranges of proteins in biological systems can reach parts per million or lower.
Similar to the international bodies that have organized to overcome complex challenges in genomics, proteomic networks like The Human Cancer Proteome Project and Human Proteome Organization are fostering cooperation and collaboration to develop and deploy better proteomic-powered tools around the world.
These networks have created multidisciplinary groups of cancer proteome scientists, pathologists, and other clinicians to standardize practices and protocols for critical research tasks, such as tissue collection, reporting, and data sharing. This collaboration is enabling the large-scale meta- and pan-cancer analyses needed to interrogate cancer at the proteome level and integrate knowledge to improve clinical decision-making and spark new clinical and translational research.
On the ground level, these efforts have produced a number of technological platforms and methodologies currently utilized for proteomic discovery and subsequent analysis. We’ve focused our attention on two that are particularly relevant to clinical application and, as Belczacka et al show through collected studies, are among the most widely applied discovery methods in use today: Liquid Chromatography Mass Spectrometry (LC-MS) and Matrix-Assisted Laser Desorption/Ionization Time of Flight (MALDI-ToF).
Chung et al succinctly compare these two strategies for identifying and profiling proteins by mass spectrometry as “bottom-up” and “top-down” proteomics.
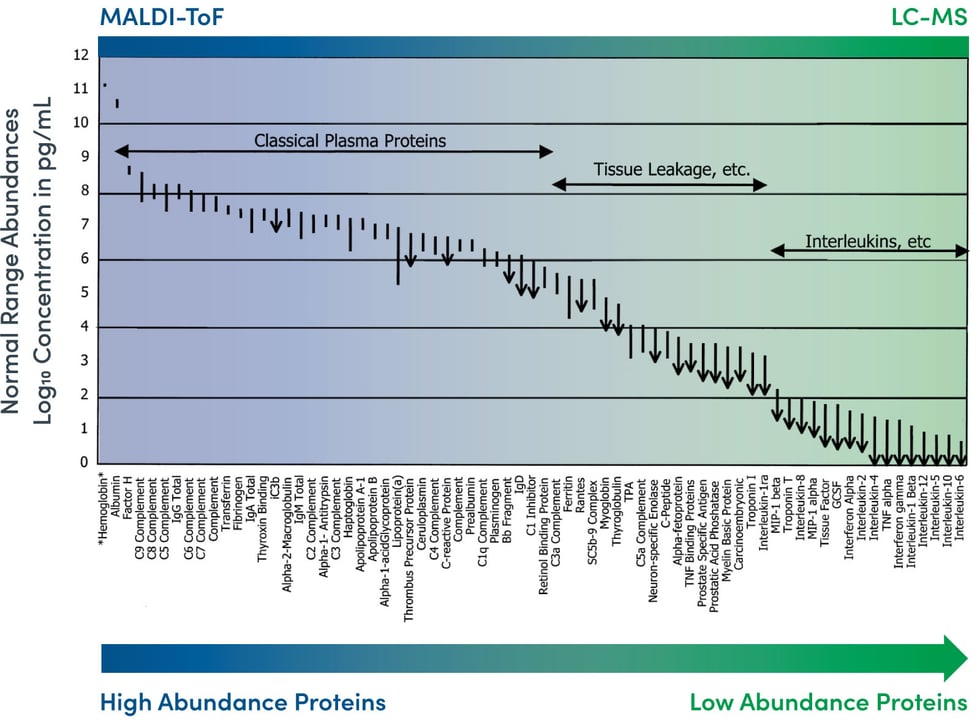
Image Source: N.L. Anderson and N.G. Anderson. The Human Plasma Proteome. Molecular and Cellular Proteomics (2002); 1:845-867.
In the “bottom-up” approach using LC-MS, a sample containing a simple or complex mixture of proteins is digested with a protease. Subsequent separation of all of the resulting peptides is performed using liquid chromatography.
In the “top-down” approach using MALDI-ToF, soft ionization allows for the optimal analyzation of larger organic molecules like peptides, lipids, and saccharides without fragmenting or decomposing them––a common drawback of traditional techniques.
Genomics and proteomics: Emerging technologies in clinical cancer research
Proteomics in cancer research: Are we ready for clinical practice?
Precision diagnostics: moving toward protein biomarker signatures of clinical utility in cancer.
Prostate cancer screening in men aged 50-69 years (STHLM3): a prospective population-based diagnostic study
Biomarker development in the precision medicine era: lung cancer as a case study
Large-scale protein identification using mass spectrometry
The building blocks of successful translation of proteomics to the clinic
Proteomics biomarkers for solid tumors: current status and future prospects